

SmartThotics: The Intelligent Alternative to Conventional Over-the-Counter Orthotics
- Tom Michaud
- 13 hours ago
- 17 min read
For more than 120 years, over-the-counter orthotics have been built around a single idea: control excessive pronation by propping up the medial longitudinal arch. The reasoning seemed obvious — if a collapsing arch drives the foot into pronation, then supporting that arch should stop it. The problem is that recent research has quietly dismantled this assumption. Arch supports, it turns out, do little to nothing to reduce the overall range of pronation. That is a serious shortcoming, because excessive pronation is strongly correlated with a wide range of foot and ankle injuries.
So how do you actually control motion? The most effective approach is to attach varus posts to the bottom of a standard orthotic shell, and these posts work best when they sit beneath both the rearfoot and the forefoot — a dual-posting technique only SmartThotics use. They also depart from conventional designs in other ways: medial and lateral flanges that increase surface area, a polyamide 11 construction favored by podiatrists, and three distinct models built for low, neutral, and high arches rather than the usual one-size-fits-the-flat-footed approach. This article walks through the science behind each of those choices.
Why Arch Supports Fall Short
Over-the-counter orthotics have been around since 1906, when Dr. Scholl introduced the first leather-covered steel arch support. Despite their rigidity, stainless steel models stayed popular until the 1970s, when manufacturers began producing arch supports from semiflexible and rigid plastics, EVA, silicone, and shock-absorbing foams. The materials changed, but the clinical goal never did: support a fallen medial longitudinal arch in the hope of preventing the pronation that occurs when the arch collapses.
Limiting excessive pronation genuinely matters. Beyond an increased risk of knee and hip pain (1,2), people who overpronate tend to have poor balance, difficulty walking, impaired athletic performance, and a greater likelihood of a range of lower-extremity injuries (2–9). The plantar fascia and Achilles tendon are especially vulnerable (8,9). One striking study found that, compared with people who have neutral arches, those with highly pronated feet are 20 times more likely to be injured during sport (10).
The catch is that, for 120 years, nobody could say with confidence whether arch supports actually reduce pronation. In 2018, Canadian researchers settled the question with a systematic review and meta-analysis of everything ever published on the subject in flat-footed populations. Their conclusion: compared with controls, arch supports do not alter the overall range or speed of pronation (11). They remain clinically useful for distributing pressure across the bottom of the foot — handy for managing bunions, metatarsalgia, and heel pain — but they simply do not control the motion they were designed to control (11).
There is a second problem with aggressively buttressing the arch: it can weaken the intrinsic foot muscles. In 2016, McClinton and colleagues reported that people with heel pain who had used orthotics long-term had significantly weaker toes than non-users (12). More recently, researchers used ultrasonography to measure arch-muscle volume before and after a 12-week trial in which young adults wore either custom orthotics or their normal shoes. By the end, the orthotic group showed 17% atrophy of the abductor hallucis and 10% atrophy of the flexor digitorum brevis, while the control group showed no change (13).

That matters, because toe weakness has been linked to bunions (14), plantar fasciitis (15), and reduced athletic performance (16) — and people with pain-free flat feet consistently have stronger toe muscles than those with painful flat feet (17,18).
There is a third downside, this one specific to runners. When the foot strikes the ground, the natural lowering of the arch stretches powerful tendons and ligaments, which store and then return that energy later in the gait cycle as elastic recoil. This "free" energy accounts for roughly 17% of the mechanical work of running (19). Block it, and you pay a metabolic price: one detailed analysis of locomotor energetics found that excessively high arch supports raise the metabolic cost of running by about 6% (20). Importantly, most of the energy from arch deflection is released in the final 25% of arch lowering — so it doesn't take much arch support to compromise running efficiency.
Varus Posting: The Real Motion-Control Mechanism

If arch supports don't alter motion, what does? Researchers turned their attention to other components of the orthotic, and the most compelling evidence points to varus posting (11,21–23). These angled wedges sit on the inner side of the orthotic, and multiple studies show they do far more than reduce foot pronation. Varus wedges also limit ankle pronation, decrease internal rotation of the knee and hip, reduce hip adduction, and significantly ease the load on the muscles responsible for decelerating pronation (22). Controlling these potentially harmful motions can lower the risk of plantar fasciitis, posterior tibial tendon injuries, Achilles tendinitis, iliotibial band syndrome, and medial tibial stress syndrome. One study even found that varus posts alone reduce valgus collapse of the knees (21) — which may lower an athlete's risk of tearing the anterior cruciate ligament.
Not all varus posts are created equal, however. The motion-control benefit is enhanced when posting is placed beneath both the rearfoot and the forefoot of the shell. As Hsu put it, "posting the rearfoot alone may not provide sufficient control during late stance" — exactly when motion control is needed most (23). This echoes earlier work by Johanson showing that rearfoot-plus-forefoot posting is the most effective way to modify excessive pronation (24).
Despite this evidence, SmartThotics remain the only over-the-counter orthotics that post both the rearfoot and forefoot. In fact, only a small fraction of over-the-counter orthotics include any posting at all — an unfortunate state of affairs given that arch supports on their own produce no change in the speed or range of pronation.
Dual posting also makes the shell dramatically stronger. Palaez and colleagues found that posting the rearfoot alone increased shell strength by 35%, but posting both the rearfoot and forefoot produced a 340% increase (25). That strength gain is clinically meaningful: it allows the orthotic to be built from the thinnest possible material, which is more comfortable and takes up less room in the shoe.
Shell Shape And Pressure Distribution
Posts control motion, but the shape of the shell determines how pressure is distributed across the bottom of the foot — and that plays a major role in preventing injury. People with low arches tend to overload the central forefoot and inner heel. Spreading pressure away from these sensitive zones becomes increasingly important with age, as the protective fat pads beneath the metatarsal heads and heels break down and chronic pain sets in.
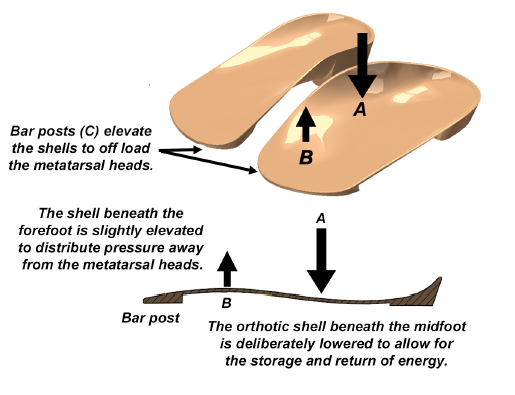
The key design principle is to support the shafts of the metatarsals, not the arch. Keeping the arch area low lets the rearfoot pronate, which is necessary for storing and returning energy and shouldn't be blocked. To protect the forefoot, the far end of the shell is elevated with a bar post that offloads the metatarsal heads. To protect the heel, a well-made shell uses an extra-deep heel cup that limits displacement of the calcaneal fat pad. This matters more than it sounds: the human heel pad is often called the world's best shock absorber, absorbing impact about 2.1 times better than Sorbothane, the most effective commercial cushioning material available (26). Containing the pad doesn't just protect the heel — it preserves the pad's own ability to store and return energy as you walk and run (26).
The Role Of Medial And Lateral Flanges in Orthotics
To distribute pressure across the entire foot, the best orthotics add medial and lateral flanges — outcroppings that significantly increase total surface area. The larger the surface area, the better the pressure distribution. On average, SmartThotics have 25% more surface area than conventional over-the-counter orthotics.
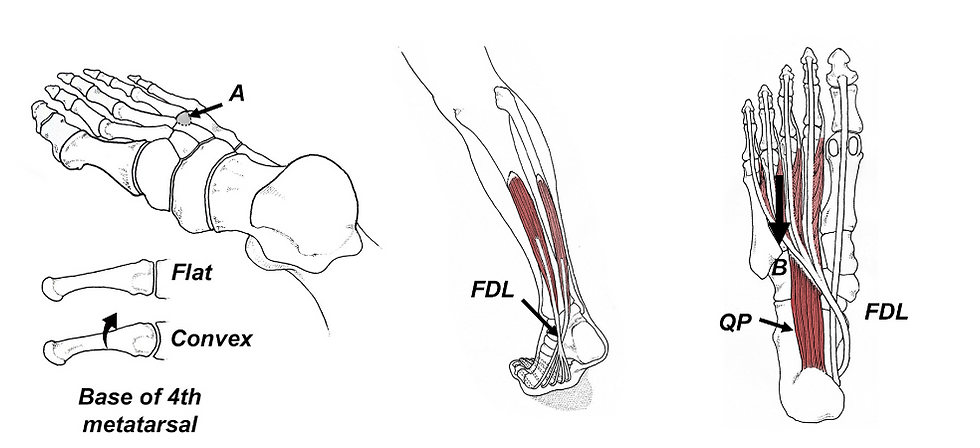
The high medial flange does something else that's rarely discussed: it helps control pronation. When a flat-footed person pronates, the arch doesn't drop straight down — it rolls inward, because of an anatomical variant in a bony shelf called the sustentaculum tali.

In flat feet, this shelf angles downward, forcing the arch to displace inward rather than vertically. On a conventional orthotic, the entire midfoot simply rolls over the top of the arch support, defeating its purpose. A large medial flange acts as a physical wall that blocks this inward roll.
Flanges also protect the plantar fascia. In a classic study published in the Journal of Bone and Joint Surgery, Kogler embedded strain gauges in the plantar fascia of cadaveric feet and loaded them onto different orthotics. Surprisingly, a standard-width orthotic actually increased plantar fascial strain — a worrying finding, since elevated strain likely raises the risk of plantar fasciitis. When the same foot was loaded onto an orthotic with medial and lateral flanges, plantar fascial tension dropped significantly (27). Whether the flanges work by preventing forefoot abduction or simply by distributing pressure over a larger area isn't fully clear, but the message is: medial flanges deserve serious consideration when prescribing orthotics for plantar fasciitis.
The Ideal Material: Polyamide 11
Material choice is one of the most important factors in an orthotic's comfort and effectiveness. While most manufacturers reach for flexible EVA foams, semiflexible plastics, or rigid graphite, the majority of foot and ankle experts prefer polyamide 11. A survey of more than 1,000 New Zealand podiatrists confirmed it: over 80% favor the material (28).
Polyamide 11 earns that preference on several fronts. Because it's derived from castor beans, it's eco-friendly, biodegradable, and hypoallergenic — and it's certified for biocompatibility, making it safe for direct, long-term skin contact. It's also remarkably strong for its weight. Unlike conventional semiflexible plastics, it resists fatigue and won't crack under the repetitive stresses of walking and running; rather than fracturing on impact like hard plastic shells, it bends and recovers. Because it lowers an average of 7 to 10 mm during midstance, it doesn't interfere with the natural shock absorption of a healthy arch — and its faster rebound rate may even help store and return energy during propulsion. Every SmartThotics model uses a 2 mm polyamide 11 shell, making them among the thinnest, lightest orthotics on the market.
Why The Best Top Cover Is No Top Cover
Because so many over-the-counter orthotics are built from stiff plastics or graphite, most come with soft foam top covers running all the way to the toes. Counterintuitively, that full-length cushioning is often a problem: thick material under the forefoot takes up space and lifts the toes into the top of the toe box, which over time can aggravate interdigital neuromas and bunions. In fact, a 2024 study by Menz and colleagues found that people with bunions strongly prefer orthotics that end just behind the metatarsal heads (29).
Because polyamide 11 is so smooth and flexible, it needs no top cover at all. That lets you drop a SmartThotic directly onto the insole already in your shoe — far simpler than removing your insole, tracing it, and cutting a new top cover to match. Top-cover materials also absorb sweat, so they discolor and smell within months. And critically, the top cover is usually the first thing to wear out: a typical cover lasts under 12 months, whereas a polyamide shell can last more than a decade. If you genuinely prefer extra cushioning and have room in your forefoot, the simple fix is an inexpensive flat top cover such as the Spenco Comfort Insole — at under $12, you won't mind replacing it yearly.
Designing For Every Foot Type
Perhaps the biggest shortcoming of the over-the-counter orthotics industry is that nearly everything is designed for flat feet. Yet an in-depth study of 600 novice runners found that while 41% had low or extremely low arches, 43% had neutral arches and 16% had high or extremely high arches (10). In other words, roughly 60% of the population is unlikely to benefit from a conventional arch support.
High-arched people — supinators — fare especially poorly with arch supports, because their arches are already elevated and the last thing they need is to be pushed higher. The injury stakes are steep: one well-designed study found runners with highly supinated feet were 76 times more likely to be injured than those with neutral arches (10). High arches strike the ground with more force and channel it along the outer side of the foot and leg, which is why supinators are roughly twice as likely to suffer stress fractures and far more prone to lateral ankle sprains, iliotibial band syndrome, hip bursitis, and fifth-metatarsal stress fractures (30,31).
Rather than supporting a rigid, already-elevated arch, the right approach for high arches is

valgus posting. Like varus posts in reverse, valgus posts sit on the outer side of the foot to coax it into rolling slightly inward, which improves shock absorption and eases stress along the lateral foot, ankle, and knee. Because people with very high arches often have a plantarflexed first ray, SmartThotics for high arches include a first-ray cutout; those with extreme arches may also benefit from adding a sub-one balance beneath the forefoot to offload the first metatarsal head and the frequently injured sesamoid bones.
People with neutral arches usually don't need any orthotic at all — but older individuals with neutral feet often prefer an unposted model with deep heel cups, wide flanges, and flat forefoot bar posts. The flanges improve balance, which becomes increasingly important with age as a predictor of falls. Those with prior nerve injuries or peripheral neuropathy can add Balance Buttons over the lateral flanges; these patented pads compress against the side of the foot when weight shifts too far outward, cueing the muscles to restore balance and helping prevent lateral falls. The neutral model also uses just a 1 mm heel elevation rather than the standard 7 mm, since excessive heel height destabilizes the ankle, stiffens the calves, and shifts weight forward.
To choose the right model, you first need to know your arch height. Researchers use various techniques, but the easiest low-tech method is to check your footprints when you step out of the shower: low arches leave excessive ground contact, while high arches leave almost none.

Getting The Fit Right: Width And Length
Because people with low arches tend to have wide feet, the low-arch SmartThotics come in standard and triple-E widths. Width matters — a too-narrow orthotic digs in along the edges, reducing both comfort and biomechanical effectiveness. A Brannock device at a shoe store is the easiest way to measure width, though you can also trace your foot at home.

Length is where most people go wrong. Instead of using standard shoe size — measured heel to longest toe — you'll get a better fit by measuring arch length: the distance from the heel to the first metatarsal head. The reason is that people with identical shoe sizes can have very different toe lengths. Someone with long toes who buys by shoe size ends up with an orthotic that projects under the metatarsal heads, often bruising the bone at their base; someone with short toes gets an orthotic that falls short, leaving the metatarsal heads unsupported and exposed to injury. A too-long orthotic is uncomfortable immediately, but a too-short one causes trouble down the road — and chronic metatarsal pain is the single most common reason people seek medical attention for foot pain (32). Notably, Payen and colleagues showed that orthotics combining rearfoot and forefoot posting, substantial medial flanges, and metatarsal pads significantly reduce pressure under the central metatarsal heads — making them especially effective for stubborn metatarsalgia (33). The orthotics in that study were nearly identical to SmartThotics, which can be fine-tuned by adding the Human Locomotion Metatarsal Pad.
In Summary
SmartThotics stand apart in the over-the-counter market because they are the only orthotics to post both the forefoot and rearfoot in their pronator and supinator models. Every model features exaggerated medial and lateral flanges that increase surface area for better pressure distribution and proprioception, plus bar posts and deep heel cups that protect the fat pads beneath the metatarsal heads and heels — common pain sources as we age. The thin polyamide 11 shell delivers long-term resilience and comfort while remaining hypoallergenic and biodegradable. On top of the standard and triple-E pronator widths, every model can be customized with peel-and-stick options — sub-one balances, metatarsal pads, balance buttons, and interdigital balances — so you can manage your individual injury pattern. Given how complex the human foot is, people deserve more than a one-size-fits-all arch support. SmartThotics let you tailor support to your needs and reach much of the benefit of costly prescription orthotics at a fraction of the price.
--
Frequently Asked Questions
Q: If arch supports don't reduce pronation, are over-the-counter orthotics useless?
No — they're just misunderstood. The 2018 meta-analysis showed that arch supports don't change the range or speed of pronation, but that doesn't make them worthless: they're still effective at redistributing pressure across the bottom of the foot, which genuinely helps with bunions, metatarsalgia, and heel pain. The real issue is that controlling motion requires a different mechanism entirely — varus posting under both the rearfoot and forefoot. So an orthotic can be valuable, but you should choose it for what it actually does rather than for an arch-supporting effect it doesn't deliver.
Q: What is the difference between varus posting and a standard arch support?
An arch support sits under the medial longitudinal arch and props it up, which feels supportive but doesn't alter the overall motion of the foot. A varus post is an angled wedge added to the bottom of the shell — on the inner side — that tilts the foot and actively reduces overpronation, ankle pronation, and internal rotation of the knee and hip. The most effective designs post both the rearfoot and the forefoot, because posting the rearfoot alone leaves the foot under-controlled in late stance. In short, the arch support is passive cushioning, while varus posting is the part that changes how the leg moves.
Q: Should high-arched runners use the same orthotics as flat-footed runners?
No, and this is one of the most common and costly mistakes. Roughly 60% of the population has neutral or high arches, and high-arched supinators in particular can be made worse by a conventional arch support, since their arch is already elevated and rigid. High arches respond better to valgus posting — a wedge on the outer side that encourages the foot to roll slightly inward, improving shock absorption and reducing lateral load. Matching the orthotic to your specific foot type matters far more than simply buying "more support."
Q: Can wearing orthotics weaken your feet, and how do you prevent it?
Long-term use of arch-supporting orthotics can contribute to atrophy of the intrinsic foot muscles — one 12-week study measured 17% wasting of the abductor hallucis and 10% of the flexor digitorum brevis. That weakness matters because it's linked to bunions, plantar fasciitis, and reduced performance. The practical fix is to treat an orthotic as a tool that manages load while you actively strengthen the foot, not as a permanent crutch, and to favor designs that keep the arch area low so the foot's own muscles and tendons still have to work and store energy.
References
Kothari A, Dixon P, Stebbins J, Zavatsky A, Theologis T. Are flexible flat feet associated with proximal joint problems in children? Gait Posture. 2016;45:204–210.
Bresnahan PJ, Juanto MA. Pediatric flatfeet—a disease entity that demands greater attention and treatment. Frontiers in Pediatrics. 2020 Feb 11;8:19.
Reilly K, Barker K, Shamley D, Newman M, Oskrochi G, Sandall S. The role of foot and ankle assessment of patients with lower limb osteoarthritis. Physiotherapy. 2009;95:164–169.
Bednarczyk E, Sikora S, Kossobudzka-Górska A, et al. Understanding flat feet: An in-depth analysis of orthotic solutions. Journal of Orthopaedic Reports. 2024 Mar 1;3(1):100250.
Ho M, Kong PW, Chong LJ, Lam WK. Foot orthoses alter lower limb biomechanics but not jump performance in basketball players with and without flat feet. Journal of Foot and Ankle Research. 2019;12(1):24.
Lee HJ, Lim KB, Yoo J, Yoon SW, Yun HJ, Jeong TH. Effect of custom-molded foot orthoses on foot pain and balance in children with symptomatic flexible flat feet. Annals of Rehabilitation Medicine. 2015;39(6):905–913.
Menz HB, Dufour AB, Riskowski JL, Hillstrom HJ, Hannan MT. Association of planus foot posture and pronated foot function with foot pain: the Framingham foot study. Arthritis Care Res. 2013;65:1991–1999.
Pazhooman H, Alamri MS, Pomeroy RL, Cobb SC. Foot kinematics in runners with plantar heel pain during running gait. Gait & Posture. 2023 Jul 1;104:15-21.
Wezenbeek E, Willems TM, Mahieu N, Van Caekenberghe I, Witvrouw E, De Clercq D. Is Achilles tendon blood flow related to foot pronation? Scandinavian Journal of Medicine & Science in Sports. 2017 Dec;27(12):1970-7.
Perez-Morcillo A, et al. Association between the foot posture index and running related injuries: a case-control study. Clinical Biomech. 2019;217-221.
Desmyttere G, Hajizadeh M, Bleau J, Begon M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: A systematic review and meta-analysis. Clinical Biomechanics. 2018 Nov 1;59:117-29.
McClinton S, Collazo C, Vincent E, et al. Impaired foot plantarflexor muscle performance in individuals with plantar heel pain and association with foot orthosis use. J Orthop Sports Phys Ther. 2016;46:681-689.
Protopapas K, Perry S. The effect of a 12-week custom foot orthotic intervention on muscle size and muscle activity of the intrinsic foot muscle of young adults during gait termination. Clinical Biomech. 2020;78.
Stewart S, Ellis R, Heath M, Rome K. Ultrasonic evaluation of the abductor hallucis muscle in hallux valgus: a cross-sectional observational study. BMC Musculoskelet Disord. 2013;14:45.
Sullivan J, et al. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot & Ankle International. 2015;36(1):37–45.
Yuasa Y, Kurihara T, Isaka T. Relationship between toe muscular strength and the ability to change direction in athletes. Journal of Human Kinetics. 2018 Oct 15;64:47.
Haelewijn N, Staes F, Vereecke E, Deschamps K. From structure to function: Biomechanical markers of symptomatic flatfoot during running and a single leg drop and hop. Clinical Biomechanics. 2025 Oct 14:106682.
Zhang X, Pauel R, Deschamps K, Jonkers I, Vanwanseele B. Differences in foot muscle morphology and foot kinematics between symptomatic and asymptomatic pronated feet. Scandinavian Journal of Medicine & Science in Sports. 2019 Nov;29(11):1766-73.
Ker RF, Bennett MB, Bibby SR, Kester RC, Alexander RM. The spring in the arch of the human foot. Nature. 1987;325:147–149.
Stearne SM, McDonald KA, Alderson JA, North I, Oxnard CE, Rubenson J. The foot's arch and the energetics of human locomotion. Scientific Reports. 2016 Jan 19;6(1):19403.
Joseph M, Tiberio D, Baird J, et al. Knee valgus during drop jumps in National Collegiate Athletic Association Division I female athletes: the effect of a medial post. Am J Sports Med. 2008;2:285-289.
Braga U, Mendonca L, Mascarenhaus R, et al. Effects of medially wedged insoles on the biomechanics of the lower limbs of runners with excessive foot pronation and foot varus alignment. Gait and Posture. 2019;74:242-249.
Hsu WH, Lewis CL, Monaghan GM, Saltzman E, Hamill J, Holt KG. Orthoses posted in both the forefoot and rearfoot reduce moments and angular impulses on lower extremity joints during walking. Journal of Biomechanics. 2014 Aug 22;47(11):2618-25.
Johanson MA, Wooden MJ, et al. Effects of three different posting methods on controlling abnormal subtalar pronation. Phys Ther. 1994;74:149–158.
Pelaez AS, Farahpour N, Griffiths IB, Moisan G. Thick shells and medially wedged posts increase foot orthoses medial longitudinal arch stiffness: an experimental study. Journal of Foot and Ankle Research. 2023 Mar 3;16(1):11.
Jorgensen U, Bojsen-Moller F. Shock absorbency of factors in the shoe/heel interaction with special focus on the role of the heel pad. Foot Ankle. 1989;9:294.
Kogler G, Veer F, Solomonidis S, Paul J. The influence of medial and lateral placement of orthotic wedges on the unloading of the plantar aponeurosis. J Bone Joint Surg Am. 1999;81:1403-1413.
Jackson A, Sheerin K, Reid D, Ganley T, Lamb B, Carroll MR. Custom Foot Orthoses: A Retrospective Analysis of 1000 Prescriptions From New Zealand Podiatrists. Journal of Foot and Ankle Research. 2025 Jun;18(2):e70044.
Menz HB, Lim PQ, Hurn SE, Mickle KJ, Buldt AK, Cotchett MP, Roddy E, Wluka AE, Erbas B, Munteanu SE. Effectiveness of footwear and foot orthoses in reducing medial metatarsophalangeal joint pressure in women with hallux valgus. Gait & Posture. 2024 Jun 1;111:156-61.
Williams D, McClay I, Hamill J. Arch structure and injury patterns in runners. Clin Biomech. 2001;16:341–347.
Michaud TC. Human Locomotion: The Conservative Management of Gait-Related Disorders. Newton Biomechanics; 2011.
Bardelli M, Turelli L, Scoccianti G. Definition and classification of metatarsalgia. Foot Ankle Surg. 2003:79-85.
Payen E, Acien M, Isabelle PL, Turcot K, Begon M, Abboud J, Moisan G. Impact of different foot orthoses on gait biomechanics in individuals with chronic metatarsalgia. Gait & Posture. 2025 May 1;118:17-24.

Tom Michaud is a chiropractor with 40 years of clinical practice and the author of the best-selling books "Human Locomotion" and "Injury-Free Running" besides being the creator of numerous diagnostic tools and exercise products such as the ToePro and Twist Disk.


Comments