

Recovery Is Not a Tool: A Systems-Based Understanding of Recovery in Sport
- Antonio Robustelli

- Apr 24
- 8 min read
In contemporary sport, the word “recovery” is sometimes used so casually that it has almost lost its meaning. Athletes and practitioners repeat that recovery is essential, yet the practical interpretation often collapses into a narrow set of routines—usually a foam roller, a massage gun, or a cold plunge. This reductionist view is incompatible with the complexity of human physiology.
A first important step is to understand that recovery is not a device/tool, nor a single technique. It is a multifactorial, system‑level process that depends on the type of stress imposed, the systems involved, and the specific mechanisms that must return to functional readiness (Thorpe, 2021).
A training session never affects only one structure or one physiological pathway. Mechanical load, metabolic stress, neural drive, autonomic balance, tissue strain, and psychological arousal all interact.
For this reason, recovery cannot be defined through a unidirectional lens. It must be understood as a coordinated process involving metabolic, neural, circulatory, respiratory, hormonal, and structural components, each with its own timeline and regulatory mechanisms. When recovery is framed this way, it becomes clear why simplistic tools cannot meaningfully restore the systems that training disrupts.
The Multifactorial Nature of Recovery
Every training stimulus produces a cascade of responses across multiple systems. High‑intensity efforts alter neuromuscular function, CNS drive, and phosphocreatine availability (Glaister, 2005). Endurance work depletes glycogen, perturbs autonomic balance, and challenges mitochondrial metabolism (Burke, van Loon and Hawley, 2017). Strength training induces muscle damage, local inflammation, and connective tissue strain (Damas et al., 2018). Even low‑intensity technical sessions influence coordination, sensory integration, and cognitive load.
These responses do not resolve through a single pathway:
Glycogen resynthesis depends on carbohydrate availability and insulin sensitivity;
Neuromuscular recovery requires restoration of excitation–contraction coupling and normalization of motor unit recruitment;
Autonomic recovery involves parasympathetic reactivation, respiratory recalibration, and cardiovascular stabilization;
Tissue regeneration requires protein synthesis, collagen turnover, and mechanotransduction;
The lymphatic system must clear metabolic by‑products and interstitial fluid;
The hormonal system must re‑establish homeostasis.
Because each system recovers through different mechanisms, at different speeds, and under different conditions, recovery must be conceptualized as a network, not a technique. This is the foundation of a systems‑based approach to human performance.
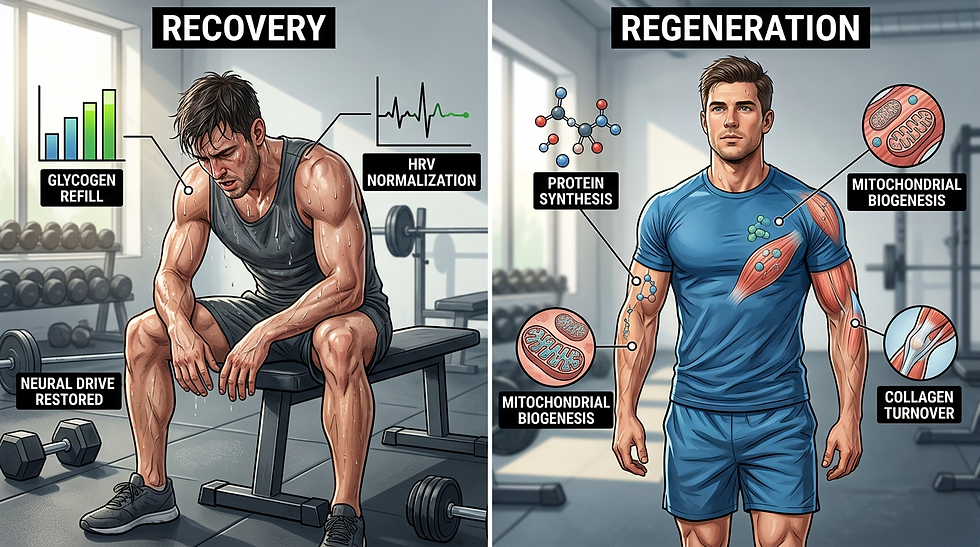
Recovery vs Regeneration: Two Distinct Processes
The terms recovery and regeneration are often used interchangeably, but they refer to fundamentally different processes. Recovery describes the restoration of acute function after a stressor. It is the process that brings the athlete back to baseline readiness—replenishing glycogen, restoring neuromuscular performance, normalizing autonomic function, and re‑establishing movement quality. Regeneration, by contrast, refers to structural repair and remodeling. It includes muscle fiber repair, collagen synthesis, tendon remodeling, mitochondrial biogenesis, and long‑term tissue adaptation (Kellmann et al., 2018).
This distinction is not semantic; it has practical consequences. Cold water immersion, for example, can reduce soreness and accelerate short‑term recovery, but chronic use around strength training may blunt hypertrophic and strength adaptations by interfering with anabolic signaling (Roberts et al., 2015). Similarly, NSAIDs may reduce pain and inflammation acutely but impair tissue regeneration and collagen synthesis when used repeatedly (Mishra et al., 1995). Recovery aims to restore function; regeneration aims to build new function. Confusing the two concepts leads to interventions that may help in the short term but compromise long‑term adaptation.
Why Recovery Is System‑Dependent and Energy‑System Dependent
Different training sessions stress different systems, and therefore the recovery process must be specific to the stressor. A high‑intensity sprint session primarily challenges the CNS, neuromuscular system, elastic tissues, and ATP‑PC energy system. The limiting factors are neural drive, tendon stiffness, and phosphocreatine resynthesis, none of which are meaningfully influenced by foam rolling or passive modalities.
In contrast, a long aerobic session stresses the cardiorespiratory system, mitochondrial metabolism, and glycogen stores. Recovery in this context depends on carbohydrate intake, hydration, autonomic recalibration, and low‑intensity movement.
Strength training produces muscle damage, local inflammation, and connective tissue strain. Recovery requires protein synthesis, collagen turnover, and adequate energy availability. Passive modalities may influence perception but do not accelerate these processes. Even technical or tactical sessions can impose cognitive and neural fatigue, requiring sleep, low‑stimulation environments, and autonomic recalibration rather than mechanical interventions.
Energy systems also dictate recovery timelines. Phosphocreatine resynthesis occurs within minutes but is influenced by oxygen availability and mitochondrial function (Bogdanis et al., 1996). Glycolytic stress produces metabolic by‑products that require circulatory clearance. Aerobic exercise affects autonomic function, requiring parasympathetic reactivation. Each energy system has its own recovery profile, and interventions must align with these physiological needs and requirements.
Why Recovery Is Not a Tool or a Button You Press
Foam rollers, massage guns, and similar devices are often marketed as recovery tools, but their effects are primarily sensory rather than physiological. They can temporarily alter perception of stiffness, modulate nociception, and increase range of motion through neural mechanisms rather than structural changes (Cheatham et al., 2015). These effects may be useful for movement preparation or subjective comfort, but they do not restore glycogen, repair muscle fibers, normalize autonomic function, or improve mitochondrial function.
The popularity of these tools reflects a broader issue: the conflation of feeling better with being recovered. Recovery is not marked byt the absence of soreness or the presence of comfort. It is the restoration of system function. A foam roller cannot accelerate glycogen resynthesis, restore CNS drive, or repair tissue microstructure. It can change how the athlete feels, but not how the system functions.
This does not make such tools useless; it simply means they should not be mistaken for recovery interventions in a strict physiological sense.
Systems‑Based Strategies to Improve Recovery Across Systems
A systems‑based approach requires matching interventions to the specific systems and mechanisms that need to recover. While the details vary, the evidence consistently supports certain strategies as effective for specific recovery targets.

Restoration of Muscle Energy Stores
Glycogen resynthesis is driven primarily by carbohydrate intake, especially in the first hours after exercise when insulin sensitivity is elevated (Burke, van Loon and Hawley, 2017). Combining carbohydrates with protein can enhance glycogen restoration and support muscle repair. Sleep also plays a central role in metabolic regulation. Active recovery at low intensity can increase blood flow and facilitate substrate delivery, although its effects are modest compared to nutrition.
Cardiorespiratory Recovery
Cardiorespiratory recovery depends on autonomic reactivation, ventilatory normalization, and fluid balance. Low‑intensity aerobic work can accelerate parasympathetic rebound and improve HRV recovery (Stanley, Peake, and Buchheit, 2013).
Breathing protocols emphasizing slow exhalation can further support autonomic regulation. Hydration and electrolyte restoration are essential, particularly after prolonged or hot‑environment sessions. Heat exposure through sauna use can enhance plasma volume and support cardiovascular adaptation, although timing relative to training matters.
CNS Recovery
CNS fatigue is influenced by neurotransmitter balance, cortical drive, and autonomic state. Sleep remains the most powerful CNS recovery tool, with both nocturnal sleep and short naps contributing to neural recalibration (Fullagar et al., 2015). Mindfulness, controlled breathing, and low‑stimulation environments can reduce sympathetic activation and support CNS restoration. Light aerobic activity may also facilitate recovery by promoting parasympathetic activity.
Neuromuscular Recovery
Neuromuscular recovery involves restoring excitation–contraction coupling (Allen, Lamb and Westerblad, 2008), normalizing muscle tone (Behm and Chaouachi, 2011), and re‑establishing efficient motor patterns through recalibration of neural drive (Enoka and Duchateau, 2008). Low‑intensity movement, targeted manual therapy, and isometric exercises can support neural drive and coordination by improving motor unit recruitment and submaximal activation patterns (Ross and Leveritt, 2001; Enoka and Duchateau, 2008). Breathing mechanics can influence rib cage dynamics and neuromuscular tone through diaphragm‑driven postural activation and modulation of intra‑abdominal pressure (Hodges and Gandevia, 2000; Kolar et al., 2012). Sleep again plays a central role, as motor learning, synaptic recalibration, and neural consolidation are fundamentally sleep‑dependent processes (Walker and Stickgold, 2004; Fullagar et al., 2015).
Tissue Regeneration
Regeneration requires adequate protein intake, typically distributed throughout the day to maximize muscle protein synthesis (Morton et al., 2018). Tendon and connective tissue regeneration benefit from mechanical loading with some help potentially coming from collagen supplementation (Shaw et al., 2017; Buchalski et al., 2026).
Mechanical loading through isometrics and eccentrics is essential for mechanotransduction and tissue remodeling. Heat exposure can increase tissue metabolism and blood flow, supporting regeneration while cold exposure and NSAIDs, however, may impair long‑term adaptation when used chronically.
Conclusion
Recovery in sport is not a routine, a device, or a trend. It is a multifactorial, system‑dependent process that requires precision, context, and an understanding of human physiology. Recovery and regeneration are distinct processes with different goals and mechanisms. Tools like foam rollers may influence perception but do not restore system function. Effective recovery requires aligning interventions with the specific systems and energy pathways stressed during training. When practitioners adopt a systems‑based approach, recovery becomes a strategic component of performance rather than a collection of disconnected techniques.
References
Allen, D. G., Lamb, G. D. and Westerblad, H. (2008) 'Skeletal muscle fatigue: cellular mechanisms', Physiological Reviews, 88(1), pp. 287–332.
Behm, D. G. and Chaouachi, A. (2011) 'A review of the acute effects of static and dynamic stretching on performance', European Journal of Applied Physiology, 111(11), pp. 2633–2651.
Bogdanis, G. C., Nevill, M. E., Boobis, L. H. and Lakomy, H. K. (1996) 'Contribution of phosphocreatine and aerobic metabolism to energy supply during repeated sprint exercise', Journal of Applied Physiology, 80(3), pp.876–884.
Buchalski, A., Jeanfavre, M., Altorelli, C. and Leff, G. (2026) 'Collagen supplementation on tendon-related structural and performance outcomes: a systematic review', Journal of Functional Morphology and Kinesiology, 11(1):130.
Burke, L. M., van Loon, L. J. C. and Hawley, J. A. (2017) 'Postexercise muscle glycogen resynthesis in humans', Journal of Applied Physiology, 122(5), pp.1055–1067.
Cheatham, S. W., Kolber, M. J., Cain, M. and Lee, M. (2015) 'The effects of self‑myofascial release using a foam roller or roller massager on joint range of motion, muscle recovery, and performance: a systematic review', International Journal of Sports Physical Therapy, 10(6), pp.827–838.
Damas, F., Phillips, S. M., Lixandrão, M. E., Vechin, F. C., Libardi, C. A., Roschel, H., Tricoli, V. and Ugrinowitsch, C. (2016) 'Early resistance training‑induced increases in muscle cross‑sectional area are concomitant with edema‑induced muscle swelling', European Journal of Applied Physiology, 116(1), pp. 49–56.
Enoka, R. M. and Duchateau, J. (2008) 'Muscle fatigue: what, why and how it influences muscle function', Journal of Physiology, 586(1), pp. 11–23.
Fullagar, H. H. K., Skorski, S., Duffield, R., Hammes, D., Coutts, A. J. and Meyer, T. (2015) 'Sleep and athletic performance: the effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise', Sports Medicine, 45(2), pp.161–186.
Glaister, M. (2005) 'Multiple sprint work: physiological responses, mechanisms of fatigue and the influence of aerobic fitness', Sports Medicine, 35(9), pp.757–777.
Hodges, P. W. and Gandevia, S. C. (2000) 'Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm', Journal of Applied Physiology, 89(3), pp. 967–976.
Kellmann, M. et al. (2018) 'Recovery and Performance in Sport: Consensus Statement', International Journal of Sports Physiology and Performance, 13(2), pp. 240–245.
Kolar, P. et al. (2012) 'Postural function of the diaphragm in persons with and without chronic low back pain', Journal of Orthopaedic & Sports Physical Therapy, 42(4), pp. 352–362.
Mishra, D. K., Friden, J., Schmitz, M. C. and Lieber, R. L. (1995) 'Anti‑inflammatory medication after muscle injury. A treatment resulting in short-term improvement but subsequent loss of muscle function', Journal of Bone and Joint Surgery, 77(10), pp. 1510–1519.
Morton, R. W. et al. (2018) 'A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults', British Journal of Sports Medicine, 54(19):e7.
Roberts, L. A., Raastad, T., Markworth, J. F., Figueiredo, V. C., Egner, I. M., Shield, A., Cameron‑Smith, D., Coombes, J. S. and Peake, J. M. (2015) 'Post‑exercise cold water immersion attenuates acute anabolic signalling and long‑term adaptations in muscle to strength training', Journal of Physiology, 593(18), pp. 4285–4301.
Ross, A. and Leveritt, M. (2001) 'Long-term metabolic and skeletal muscle adaptations to short-sprint training: implications for sprint training and tapering', Sports Medicine, 31(15), pp. 1063–1082.
Shaw, G., Lee‑Barthel, A., Ross, M. L., Wang, B. and Baar, K. (2017) 'Vitamin C–enriched gelatin supplementation before intermittent activity augments collagen synthesis', American Journal of Clinical Nutrition, 105(1), pp.136–143.
Stanley, J., Peake, J. M. and Buchheit, M. (2013) 'Cardiac parasympathetic reactivation following exercise: implications for training prescription', Sports Medicine, 43(12), pp.1259–1277.
Thorpe, R. (2021) 'Post-exercise recovery: cooling and heating, a periodized approach', Frontiers in Sports and Active Living, 3:707503.
Walker, M. P. and Stickgold, R. (2004) 'Sleep-dependent learning and memory consolidation', Neuron, 44(1), pp. 121–133.

Antonio Robustelli is the mastermind behind Omniathlete. He is an international high performance consultant and sought-after speaker in the area of Sport Science and Sports Medicine, working all over the world with individual athletes (including participation in the last 5 Olympics) as well as professional teams in soccer, basketball, rugby, baseball since 23 years. Currently serving as Faculty Member and Programme Leader at the National Institute of Sports in India (SAI-NSNIS).



Comments